Controlling Receivables in Today’s Podiatric Practice
No matter how long you have been in practice, the trends and points discussed here will pertain to you. Please keep in mind that this article was not composed as a negative rant about the state of healthcare, but instead as a reminder that private practice growth and success is still possible in today’s changing climate through diligence, attention to detail and thorough management of metrics.
Receivable management includes monitorization of aging insurance and patient balances, follow-up and documentation from in-house billers and revenue cycle management (RCM) companies, timely filing, rejection and denial rates, clearinghouse efficiencies, payer trends, and patient responsiveness to statements. In order to keep abreast of the financial status of their practices, it is imperative that physicians (practice owners) and the parties responsible for revenue cycle management meet frequently to review financial reports.
We begin with A/R (Accounts Receivable) reports as they are amongst the most telling. These should include current A/R (0-30 days) as well as aging (31-60), (61-90), (91-120) and (121+ days) and should then be broken down into total A/R as well as patient versus insurance aging. Once you have a picture of what these buckets include, additional reports should be generated to show problem payers and trends that may be affecting your bottom line. If you are not meeting regularly or at least receiving reports on a monthly basis from your biller, how do you know the status of receivables (monies owed to you) in your practice? See Figure 1 at the end of this article for “healthy” A/R information).
The next areas to look at are charges and collections. When doing so, there are a few specifics to consider. First, how long are we waiting for reimbursement? This can be determined by running an aging report broken down by specific payer. Medicare will pay “clean claims” in about two weeks while commercial payers tend to take longer even though they have the ability to pay within a week. Keep an eye out for those who take excessively long to pay and find out the reason. It may be something as simple as an incorrect “Payer ID” or an EDI Enrollment issue. Delayed payments can often be related to inefficiencies in your (and your team’s) daily practices or a lack of consistency in claims submission and payment posting by your biller or RCM company. Commonly, physicians find themselves falling behind with chart notes, leading to incomplete encounters (documentation and coding), resulting in delayed submission of claims. Be very careful of this issue as some private payers have timely filing limits of 90 or sometimes even 60 days. Although Medicare still allows twelve months to file a claim, Medicare replacement plans administered by private payers follow private payer timely filing limits. This can be detrimental to cash flow if not closely monitored.
Although collection rates will vary depending on charged amounts (per service) and payer mix, it is important to establish a baseline in order to determine if your percentage is within normal limits (for your individual practice). For example, if you bill out/charge twice the Medicare allowable for most services, your collection rate should run on average between 45-55%. Collection rates should be run monthly, quarterly and annually to provide accurate numbers for your practice. Keep in mind that dollars collected for a given month are at times suggestive of charges from the previous month (if you saw a large number of patients in June to prepare for a week vacation in early July, your July collections would be high compared to July charges and inflate your percentage temporarily).
Along with charges and collections, it is important to keep a close eye on rejection rates. This assures that only “clean claims” are being submitted. If your rejection rate is greater than 3% you may find issue with any of the following not being “scrubbed.” First, patient eligibility and benefits must be checked on each patient (most importantly to determine if the patient has active coverage at the time of visit and also to discover if they have a plan that carves out podiatry services or has an exceptionally high copay or deductible). Next, are coding and charges being entered according to payer guidelines (Local Coverage Determination)? Many rejections can be avoided by paying closer attention to detail. Simple human error is the main cause of delayed payments including incorrect place of service (POS) codes, missing referring provider information (including date last seen on both claim and chart note for Medicare patients), and basic demographic information entered with transposed numbers or misspelled names (not spelled as on insurance card). Taking just a few extra moments to “scrub” can save weeks (if not longer) of chasing reimbursement. See Figure 2 at the end of this article for examples of recommended reports.
Sometimes claims are not rejected or accepted and become “stuck” somewhere in between (not passing through the clearinghouse to the payer). Do you know if this happens to any of the claims in your practice? If you are unsure, is someone in your practice or billing team responsible for checking? In fact, how do you know if encounters/claims for all patients who require one (insurance billed visits) have been generated at all? Once a week a report should be obtained from the scheduler showing how many patients were treated compared to the number of encounters created and claims submitted (claims should be submitted within 48 hours of treatment or chart note completion). A weekly report should also be run to compare submitted claims to accepted claims. Clearinghouses have frequent “glitches” that sometimes aren’t communicated to providers or billers until a major issue has been caused.
Provided that we are putting forth our best effort to keep up with charting, submitting clean claims, following up with slow paying insurers, and controlling our insurance collection rates, there is still the issue of patient responsibility. Each year as premiums rise, copayments increase, and deductibles skyrocket, it is imperative to monitor patient aging and collect monies owed as well as any outstanding balances at the time of service. The phrase “Strike while the iron is hot” is more pertinent than ever in the business of medicine. All staff members involved in the check in process should be aware of patients with previous balances as well as those with out of pocket expenses which may arise from each visit. Checking eligibility and benefit information is the best way to determine coverage (or lack there-of) and to educate patients ahead of their visit regarding monies which may be owed (no one likes to be surprised with a large bill). When patients present to the office with a previous balance, staff should be prepared with a printed statement which clearly outlines the service date and amount due. On an individual basis (depending on condition) it should be pre-determined if rescheduling is necessary if a patient refuses to pay. If you continue to treat patients with outstanding balances, how do you expect to stay in business?
Non-returning patients (discharged as PRN or who fail to present for follow-up care) who ignore statements is a common problem for many practices. However, it is a problem that can be significantly improved by implementing a few simple changes resulting in time, money and reputation savings. Instead of sending statement “batches” every thirty days and causing upheaval at your front desk, try sending smaller batches more often and control the influx of billing questions and calls. Prior to each batch being mailed or emailed, take a look and see who is receiving a statement and the amount owed. If it costs a practice an average of seven dollars per mailed statement, why then would we mail out statements totaling less than that? For each patient with an outstanding balance of less than ten dollars, check and see if the patient has an upcoming appointment and collect at check-in. If the patient does not have an upcoming appointment, call them, make some small talk leading to casual mention of their balance and ask them if they would like to take care of it now or mail in a check tomorrow (documenting the patient’s response).
The same method can be very effective in collecting from delinquent patients with large balances. In these cases, your staff member is on a mission. That mission involves first, confirming the patient’s mailing or email address (to make sure a data entry error has not caused the delay in payment); second, to alert the patient (as it has been brought to the staff member’s attention by your “billing department”) that three statements have been sent with no response; and third, to relay concern to the patient that they will soon be turned over to collections if payment is not made.
When dealing with patient responsibility, it is you (your practice) and the patient against the big bad insurance companies and sometimes even the “billing department” (in-house or outsourced) in order to keep a separation between a positive patient care experience and monies owed. It is all perception and the key to avoiding large, overdue patient balances begins before they are ever treated. Weed them out by adhering to your financial policy (you know the part where it says “copayments and other out of pocket expenses are due at the time of service” or “a 24-hour cancellation notice is required to avoid a $30 charge”). If you clearly state your policies upon the initial phone call, again during the appointment reminder, present it to them in person upon arrival, and they refuse to pay, don’t allow them to become your patient (and soon your financial burden). Simple as that.
Not so simple are the causes of inflated A/R resulting in an inaccurate financial snapshot of the practice. This may be caused by missed adjustments (such as in cases where Medicaid is secondary) or even when billing for orthotics. For example; If you charge $350 per unit for L3000 (a pair; 2 units is billed out at $700) and the allowed amount is $200 per unit. The patient should not receive a statement for a $300 balance. It seems obvious, but a biller who is not familiar with podiatry services may not be aware.
Inexperienced billers may also be causing your aging buckets to become larger than necessary due to lack of follow-up. Often times rejections or denials are “touched” meaning an initial communication is made to determine that a claim needs to be resubmitted due to simple omission of a modifier and is never “touched” again. We see the biller’s notes recorded immediately following the denial that state; “4/10/19, called and spoke with Kathy at BC, she said that once we re-submit the claim with the appropriate modifier, we should see a response within 10 business days.” It is now the middle of July and the claim is still marked as re-submitted without response from Blue Cross and no follow up communication has taken place. Had the biller set up a simple alert or reminder to follow up by April 30th (providing ample time for insurance reprocessing) we could have avoided this exceedingly long delay in payment. Keep in mind that most payers bank on the fact that practices and billers are too busy to follow-up resulting in an increasing number of claims that go unpaid.
In addition to human inefficiency and error, inflated A/R may also be due to issues with electronic transmission, submission or deposit agreements. It is imperative to assure that all are properly in place in order to receive the most accurate information about each line item on your claims. In other words, just because you have an EDI (Electronic Data Interchange) agreement set up with Blue Cross of NY, your ERA (Electronic Remittance Advice) may not be set up properly causing delays in payment and posting. If you are still receiving paper checks rather than EFT (Electronic Funds Transfer) there is most likely a disconnect between monies received and applied payments. All payers that accept electronic submission (most do) should be set up that way. EFT must be set up separately from ERA ensuring receipt of electronic EOBs (Explanation of Benefits) rather than having to search or call for a paper EOB when you realize a check from Blue Cross was received and deposited without knowing which patients, claims, or line items to apply payments to. If you outsource billing, this can be especially problematic as without an EOB, funds cannot be applied and 0$ “paid” line items are often adjusted off inappropriately.
When speaking of EOBs and line item payments, physicians and billers often overlook the importance of individual fee schedules. We know that CMS (Medicare and Medicaid) fee schedules are posted online according to locality, but what about commercial payers? Once you are initially credentialed and receive your fee schedule (this is part of your contract with the payer and you are entitled to review it) another fee schedule is almost never provided. Each year an updated fee schedule should be requested from provider relations representatives (they do exist, you just have to do some investigating to find out how to contact them). This schedule should be provided to your biller so that expected allowed amounts can be updated within your practice management system. It is also a good idea to review charges associated with common procedures to assure that your charges are not too close to or less than allowed amounts (it happens all the time). Some physicians will have modified charge amounts for specific payers (who may allow significantly more or less than Medicare). See Figure 3 at the end of this article for symptoms of unmanaged receivables.
Major contributors to cash flow headaches including payers who seem to change the rules as they go without notification. If you choose to continue contracting with these plans, it is crucial to monitor closely and make sure all physicians and team members involved in documentation, billing and coding are aware as changes happen. Some examples of changes that you may be unaware of are: Medicaid of Utah decide to stop paying podiatrists for E/M visits above level two (for new or existing patients), Blue Cross of Michigan discontinued orthotic coverage and has since reversed their decision, several commercial payers reduced their timely filing limits, workers compensation in many states makes it increasingly more difficult to get paid for services provided and takes far longer to reimburse than most. At the end of each year, a plan of action should be developed for handling problem payers in your practice. This plan may vary from discontinuing contracts or limiting new patients insured by these plans.
In conclusion, if you are not monitoring receivables closely you can be certain that a percentage of services you are providing (billing for) are not being paid. If you are not meeting and communicating with your biller or RCM company on a consistent basis, you may be unaware of poor performance and follow through resulting in large amounts of unrelinquishable funds left on the table. On a positive note, with detailed reporting and metric management there is always something that can be done to improve the situation. Whether you are new to practice or a seasoned veteran, developing systems and creating accountability as soon as possible is key. Learning how to generate and analyze basic financial reports as well as becoming familiar with reading and understanding EOBs will allow you to maintain better control of your practice finances. If you require assistance with the management and improvement of receivables or your overall practice health, please visit www.pinnaclepa.com. We are here to help.
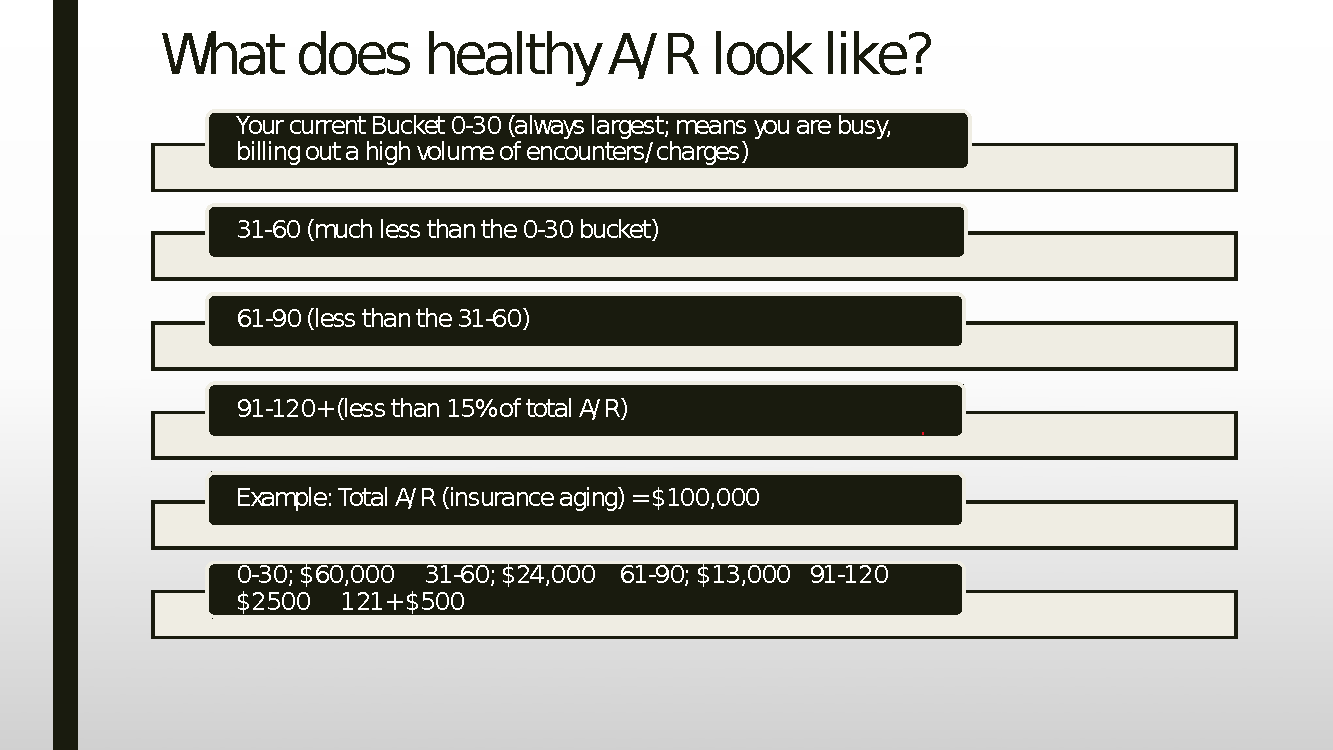
Figure 1- “Healthy” A/R information
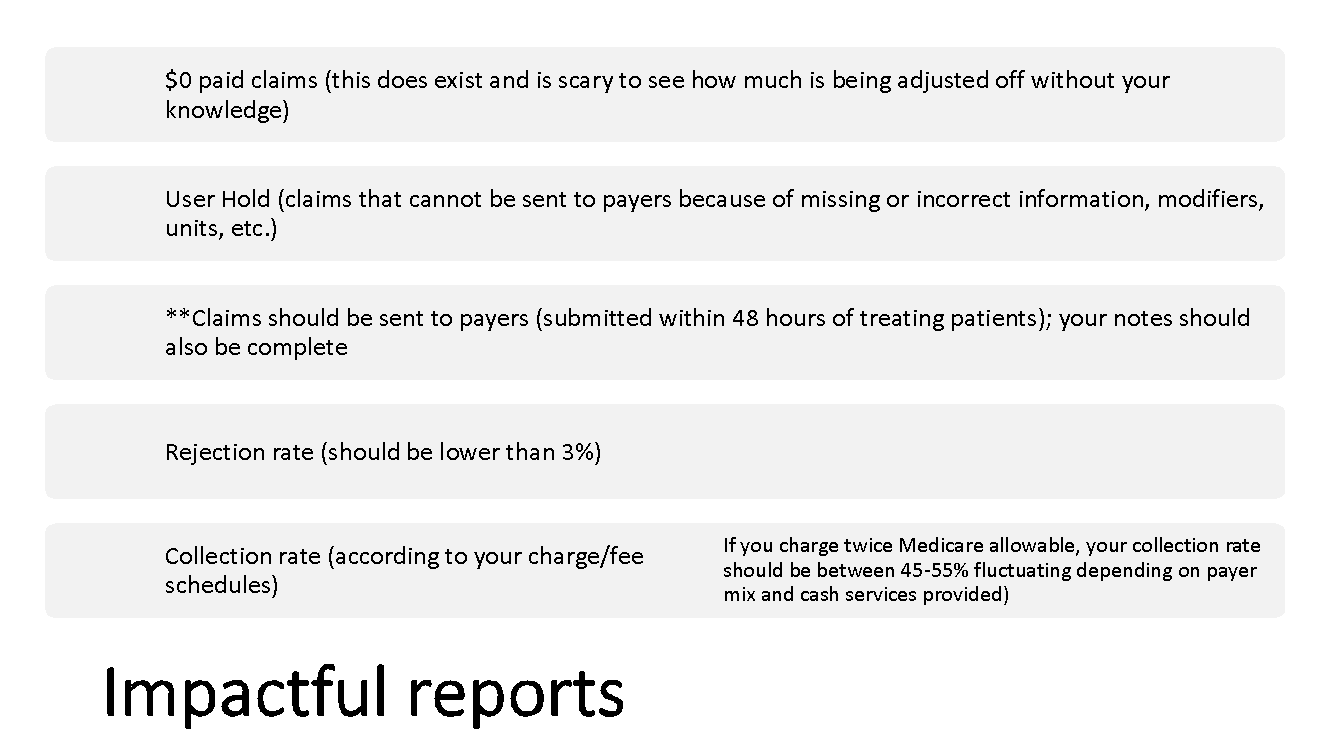
Figure 2- Recommended and Impactful Reports
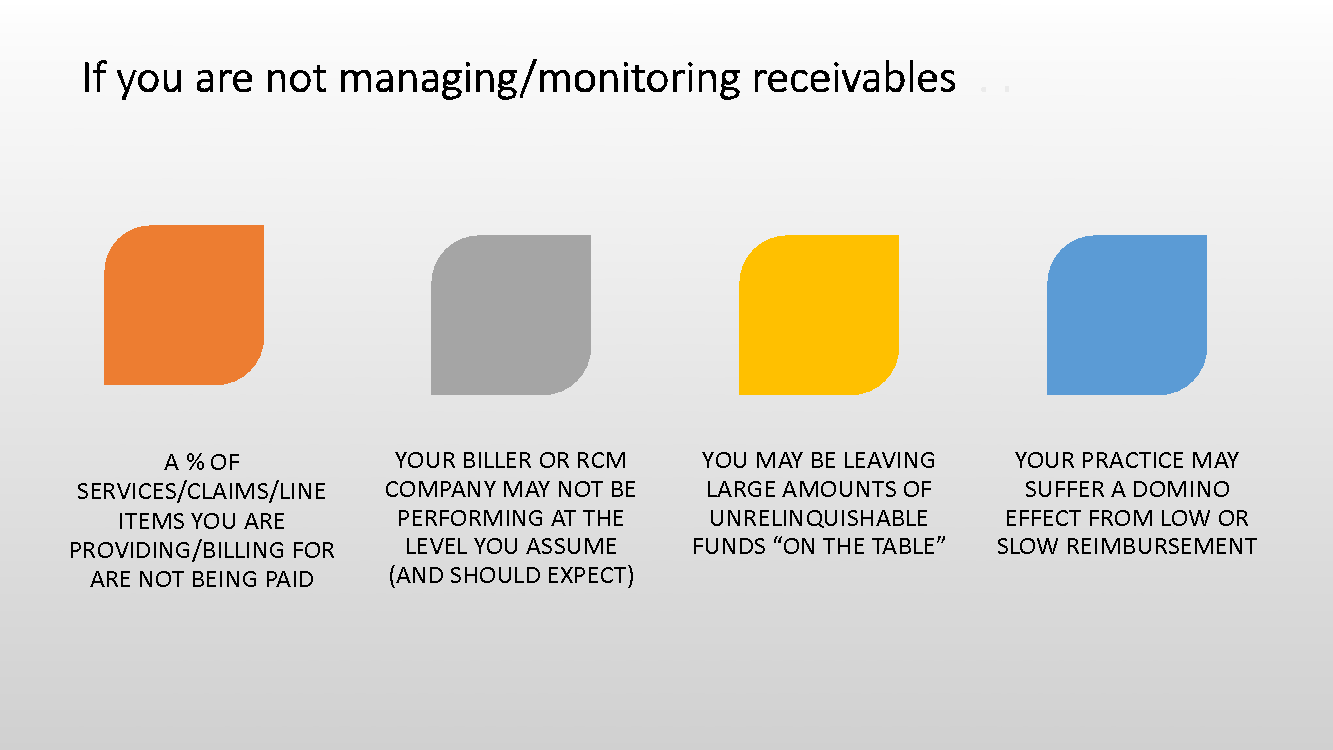
Figure 3- Symptoms of Unmanaged Receivables
1 Comment
Leave a Comment
You must be logged in to post a comment.
[…] Click here to read the full article “Controlling Receivables in Today’s Podiatric Practice” […]